
Conditions & Treatments General Urology Urologic Cancer Bladder Cancer Treating Bladder Cancer Surgical Treatment of Bladder Cance ...
Surgical Treatment of Bladder Cancer
Our bladder cancer specialists utilize the most advanced surgical and reconstructive techniques for the best outcomes.
- TURBT (transurethral resection of bladder tumor) – This is an endoscopic surgery performed to remove a bladder tumor. A surgical telescope is passed via the urethra into the bladder and an electrosurgical loop is used to remove the tumor and fulgurate the base. This procedure is not only therapeutic in removing all visible tumors, but it is also diagnostic in that it allows the physician to collect tissue for a pathologist to evaluate the histology, grade, and stage of the tumor.
- Radical Cystectomy – This technique involves the total removal of the bladder. The procedure usually also involves the removal of lymph nodes and other sexual organs (the prostate and seminal vesicles in men; the uterus, fallopian tubes, ovaries, and part of the vagina in women). Radical surgical treatment is often recommended for patients with invasive bladder cancer, in select patients with high-risk, non-invasive cancer, and when other non-surgical therapies have not been successful. A radical cystectomy can be performed as a traditional open surgery or robotically. Based on your health history and type of bladder cancer, your surgeon will determine if you are an appropriate candidate for a robotic cystectomy.
- Urinary Diversion – For patients who receive a radical cystectomy, your surgeon will perform a procedure called a urinary diversion, which provides your body with a way to potentially store and remove urine in the absence of your bladder.
Types of Urinary Diversion
-
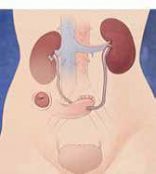 Ileal conduit (ileal loop) – This is the most common and simplest type of urinary diversion.
A segment of the intestine (ileum) is used to create a pipe or pathway,
connecting the ureters to the outside of the body through an opening in
the abdominal wall. The opening is called a stoma and is covered with
a bag that collects urine as it drains from the ileal conduit. This diversion
is the easiest for many patients and has no physical limitations, although
some patients find that the bag interferes with self-image.
Ileal conduit (ileal loop) – This is the most common and simplest type of urinary diversion.
A segment of the intestine (ileum) is used to create a pipe or pathway,
connecting the ureters to the outside of the body through an opening in
the abdominal wall. The opening is called a stoma and is covered with
a bag that collects urine as it drains from the ileal conduit. This diversion
is the easiest for many patients and has no physical limitations, although
some patients find that the bag interferes with self-image.
-
 Continent (catheterizable) reservoir – In this procedure, an internal pouch is created from a portion
of the intestines and the ureters are repositioned to drain into this
pouch. A stoma is created using a piece of the intestine and brought out
through an opening in the navel. Unlike the ileal conduit, no bag is used.
A one-way valve is created to keep the urine inside of the pouch. Then,
a catheter must be inserted into the stoma every four to six hours to
drain urine from the pouch.
Continent (catheterizable) reservoir – In this procedure, an internal pouch is created from a portion
of the intestines and the ureters are repositioned to drain into this
pouch. A stoma is created using a piece of the intestine and brought out
through an opening in the navel. Unlike the ileal conduit, no bag is used.
A one-way valve is created to keep the urine inside of the pouch. Then,
a catheter must be inserted into the stoma every four to six hours to
drain urine from the pouch.
-
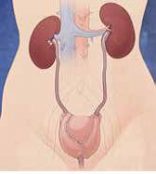 Neobladder (new bladder) – A segment of the intestine is harvested and used to create a new
“bladder.” Your surgeon will reconfigure a segment of bowel
into a spherical pouch and attach the pouch to the urethra. Urine is able
to drain from the kidneys to the ureters, to the pouch, and through the
urethra in a way that is similar to the normal passing of urine. With
the neobladder, patients do not have to wear an appliance or bag and do
not have a dramatic change in body image, although incontinence, particularly
at night, is one of the disadvantages. This surgery is more complex and
patients have to “re-learn” how to urinate. In addition, many
patients have to catheterize the neobladder via the urethra. With any
surgical procedure, there are advantages as well as risks and complications
that may arise. Your urologist will discuss your surgical options in detail
with you to help you make the most informed decision.
Neobladder (new bladder) – A segment of the intestine is harvested and used to create a new
“bladder.” Your surgeon will reconfigure a segment of bowel
into a spherical pouch and attach the pouch to the urethra. Urine is able
to drain from the kidneys to the ureters, to the pouch, and through the
urethra in a way that is similar to the normal passing of urine. With
the neobladder, patients do not have to wear an appliance or bag and do
not have a dramatic change in body image, although incontinence, particularly
at night, is one of the disadvantages. This surgery is more complex and
patients have to “re-learn” how to urinate. In addition, many
patients have to catheterize the neobladder via the urethra. With any
surgical procedure, there are advantages as well as risks and complications
that may arise. Your urologist will discuss your surgical options in detail
with you to help you make the most informed decision.